Correction of a Key Study: No Evidence of “Gender-Affirming” Surgeries Improving Mental Health
In October 2019, the American Journal of Psychiatry (AJP) published a study from the Karolinska Institute in Sweden, and the Yale School of Public Health which reported that “gender-affirming" surgeries for gender dysphoric patients are associated with improved mental health outcomes (1). Looking at mental health utilization in the year 2015, a retrospective analysis showed that the more time passed since surgery, the fewer mental services were utilized by patients, with an average 8% reduction in mental health utilization for each year following surgery. From this, the study concluded that surgery has a beneficial effect on mental health, and that benefits continue to accrue over time. However, following a reanalysis of the data, this conclusion has now been officially corrected to indicate that there is “no advantage of surgery.”
Original Study by Bränström & Pachankis (2019)
The study (1) analyzed health records of 2,679 Swedes diagnosed with gender dysphoria between 2005 and 2015 to determine whether hormonal or surgical treatments improved their mental health over time. To approximate mental health outcomes, the authors relied on the count of mental health visits, psychiatric medication prescriptions, and hospitalizations following suicide attempts. It was presumed that the fewer “mental health events” a person experienced, the better their mental health.
While the authors found no evidence of benefits of hormonal treatments (adjusted odds ratio=1.01, 95% CI=0.98 - 1.03), they noted a statistically significant relationship between time since surgery and mental health status (adjusted odds ratio=0.92, 95% CI=0.87 - 0.98). Specifically, the researchers observed that as of 2015, patients who had surgeries further in the past had better mental health than patients whose surgeries were more recent. This “longitudinal association between gender-affirming surgery and reduced likelihood of mental health treatment” was interpreted by the authors as the evidence of a positive, time-release-like effect of “gender-affirming” surgery. The authors opined that this finding should “lend support to the decision to provider gender-affirming surgeries to transgender individuals who seek them.” The conclusions of the study were widely publicized by mass media outlets. The study also made a rapid and significant impact on clinical and public health education.
Vigorous Debate Leads to Correction of Key Finding
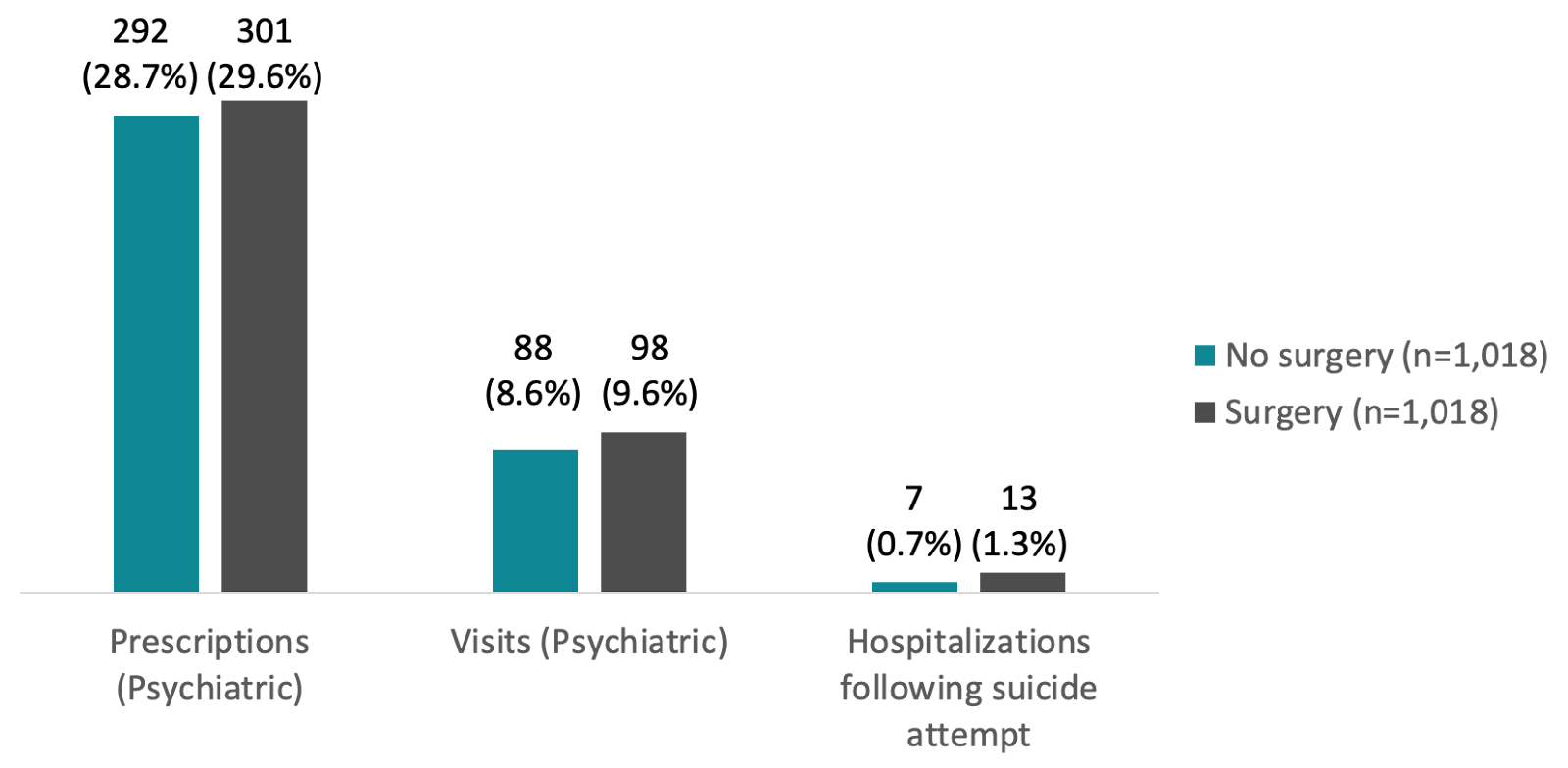
After the study was published, many researchers and scientists (including some SEGM advisors) alerted the AJP to multiple serious methodological problems that challenged the study’s conclusion. In response, the AJP editor requested an independent statistical review of the data, which led to a reanalysis of the data and an official correction (2,3). When gender dysphoric patients who received surgeries were compared to those who did not have surgeries, there was no statistically significant difference in their mental health utilization (Figure 1).
Nine months after the study’s original publication, the AJP stated, “the results [of the reanalysis] demonstrated no advantage of surgery in relation to subsequent mood or anxiety disorder-related health care visits or prescriptions or hospitalizations following suicide attempts” (2).
Figure 1. 2015 Mental Health Services Utilization Among Patients Diagnosed with Gender Dysphoria in Sweden Between 2005 and 2015 by "Gender-Affirming" Surgery Status
Range of Interpretations
The results of the Bränström & Pachankis original analysis (2019) and their re-analysis (2020) may be interpreted in a number of ways. They include the possibility that "gender-affirming" surgeries improve mental health, worsen mental health, or that the data are insufficient to draw conclusions about the impact of hormonal and surgical interventions on mental health.
SEGM Position
It is SEGM’s view that the data presented in the original study and the subsequent re-analysis do not support the claim of an expected "reduction in mental health treatment as a function of time since completing such treatment” (14). After the reanalysis of the data, we conclude the following:
- The mental health needs of people suffering from gender dysphoria are significantly greater than those of the general population, which confirms previous research
- No mental health benefit of hormonal interventions was demonstrated
- No mental health benefit of "gender-affirming" surgery was demonstrated
- Specific to the question of longitudinal association between time from surgery and mental health outcomes, due to unaddressed study design limitations, no improvement of mental health with time after surgery was demonstrated
- Despite the higher rate of suicide attempts requiring hospitalization in the "surgery" group, the study design precludes the assertion that "gender-affirming" surgery is harmful
Closing Thoughts
We applaud the AJP and the study authors for addressing some of the concerns expressed by researchers and scientists regarding the flawed methodology of the study and the problematic conclusion, and for issuing a correction to the study’s key finding. We are heartened that the Karolinska Institute, home of the study’s primary author, promptly acknowledged the correction. More recently, Yale University's School of Public Health, the home of the study’s other author, has also replaced its news story lauding the original study findings with an acknowledgement of the correction.
Unfortunately, the original study with its misleading title and incorrect conclusion continues to be available on the AJP's website. The original, uncorrected study also remained part of Continuing Medical Education courses by Medscape, which is relied on by clinicians worldwide for accurate, evidence-based information. [Update November 4th, 2020: We thank Medscape for taking our concern seriously and for initiating the process of issuing a correction, as well as notifying the clinicians who have already received the CME credit associated with this study of the significant change in the study's main conclusion.] The Association of Schools and Programs of Public Health, disseminating information to 180 schools and programs in public health, has yet to correct its publication.
Gender dysphoric patients and the clinicians who care for them need quality, accurate information to make informed decisions. This is especially true for adolescents and young adults, who are currently the vast majority of patients presenting to gender clinics, and whose decisions will have profound, life-long implications. It’s critical that the AJP update the original study’s title and conclusion in order to reflect this critical correction. It is also urgent that all organizations that had disseminated the incorrect conclusions publicize the fact that the conclusions have now been corrected, and that any treatment guidelines or recommendations based on the original finding are promptly updated to reflect this new information.
References
- Bränström, R., & Pachankis, J. (2019). Reduction in Mental Health Treatment Utilization Among Transgender Individuals After Gender-Affirming Surgeries: A Total Population Study. American Journal Of Psychiatry, 177(8), 727-734. https://doi.org/10.1176/appi.ajp.2019.19010080
- Correction to Bränström and Pachankis. (2020), 177(8), 734-734. https://doi.org/10.1176/appi.ajp.2020.1778correction
- Kalin, N. (2020). Reassessing Mental Health Treatment Utilization Reduction in Transgender Individuals After Gender-Affirming Surgeries: A Comment by the Editor on the Process. American Journal Of Psychiatry, 177(8), 764-764. https://doi.org/10.1176/appi.ajp.2020.20060803
- Anckarsäter, H., & Gillberg, C. (2020). Methodological Shortcomings Undercut Statement in Support of Gender-Affirming Surgery. American Journal Of Psychiatry, 177(8), 764-765. https://doi.org/10.1176/appi.ajp.2020.19111117
- Curtis, D. (2020). Study of Transgender Patients: Conclusions Are Not Supported by Findings. American Journal Of Psychiatry, 177(8), 766-766. https://doi.org/10.1176/appi.ajp.2020.19111131
- Landén, M. (2020). The Effect of Gender-Affirming Treatment on Psychiatric Morbidity Is Still Undecided. American Journal Of Psychiatry, 177(8), 767-768. https://doi.org/10.1176/appi.ajp.2020.19111165
- Malone, W., & Roman, S. (2020). Calling Into Question Whether Gender-Affirming Surgery Relieves Psychological Distress. American Journal Of Psychiatry, 177(8), 766-767. https://doi.org/10.1176/appi.ajp.2020.19111149
- Ring, A., & Malone, W. (2020). Confounding Effects on Mental Health Observations After Sex Reassignment Surgery. American Journal Of Psychiatry, 177(8), 768-769. https://doi.org/10.1176/appi.ajp.2020.19111169
- Wold, A. (2020). Gender-Corrective Surgery Promoting Mental Health in Persons With Gender Dysphoria Not Supported by Data Presented in Article. American Journal Of Psychiatry, 177(8), 768-768. https://doi.org/10.1176/appi.ajp.2020.19111170
- Van Mol, A., Laidlaw, M., Grossman, M., & McHugh, P. (2020). Gender-Affirmation Surgery Conclusion Lacks Evidence. American Journal Of Psychiatry, 177(8), 765-766. https://doi.org/10.1176/appi.ajp.2020.19111130
- “Why has mental illness increased among children and young people in Sweden?” Swedish (”Varför har psykiska ohälsan ökat hos barn och unga ?”) National Health Agency, 2018. Manuscript number: 18023-2. www.folkhalsomyndigheten.se https://www.folkhalsomyndigheten.se/contentassets/628f1bfc932b474f9503cc6f8e29fd45/varfor-psykiska-ohalsan-okat-barn-unga-18023-2-webb-rapport.pdf
- Bremberg, S. & Dalman, C.. (2015). “Mental illness and psychiatric conditions in children and adolescents”. Swedish (”Psykisk ohälsa och psykiatriska tillstånd hos barn och unga”). Ministry of Health and Social Affairs, Swedish Research Council for Health, Working Life and Welfare. www.forte.se. Originally https://forte.se/app/uploads/2014/12/kunskapsoversikt-begrepp.pdf, available at https://web.archive.org/web/20200216123237/https://forte.se/app/uploads/2014/12/kunskapsoversikt-begrepp.pdf
- Dhejne, C., Lichtenstein, P., Boman, M., Johansson, A., Långström, N., & Landén, M. (2011). Long-Term Follow-Up of Transsexual Persons Undergoing Sex Reassignment Surgery: Cohort Study in Sweden. Plos ONE, 6(2), e16885. https://doi.org/10.1371/journal.pone.0016885
- Bränström, R., & Pachankis, J. (2020). Toward Rigorous Methodologies for Strengthening Causal Inference in the Association Between Gender-Affirming Care and Transgender Individuals’ Mental Health: Response to Letters. American Journal Of Psychiatry, 177(8), 769-772. https://doi.org/10.1176/appi.ajp.2020.20050599
- Kaltiala-Heino, R., Bergman, H., Työläjärvi, M., & Frisen, L. (2018). Gender dysphoria in adolescence: current perspectives. Adolescent Health, Medicine And Therapeutics, Volume 9, 31-41. https://doi.org/10.2147/ahmt.s135432