Rethinking Youth Gender Medicine:
Charting a Path Forward
November 5-7 | Washington, DC
Our aim is to promote safe, compassionate, ethical and evidence-informed healthcare for children, adolescents, and young adults with gender dysphoria
Early-bird registration is now open for SEGM's 2026 conference
Latest from SEGM
“
SEGM in Media








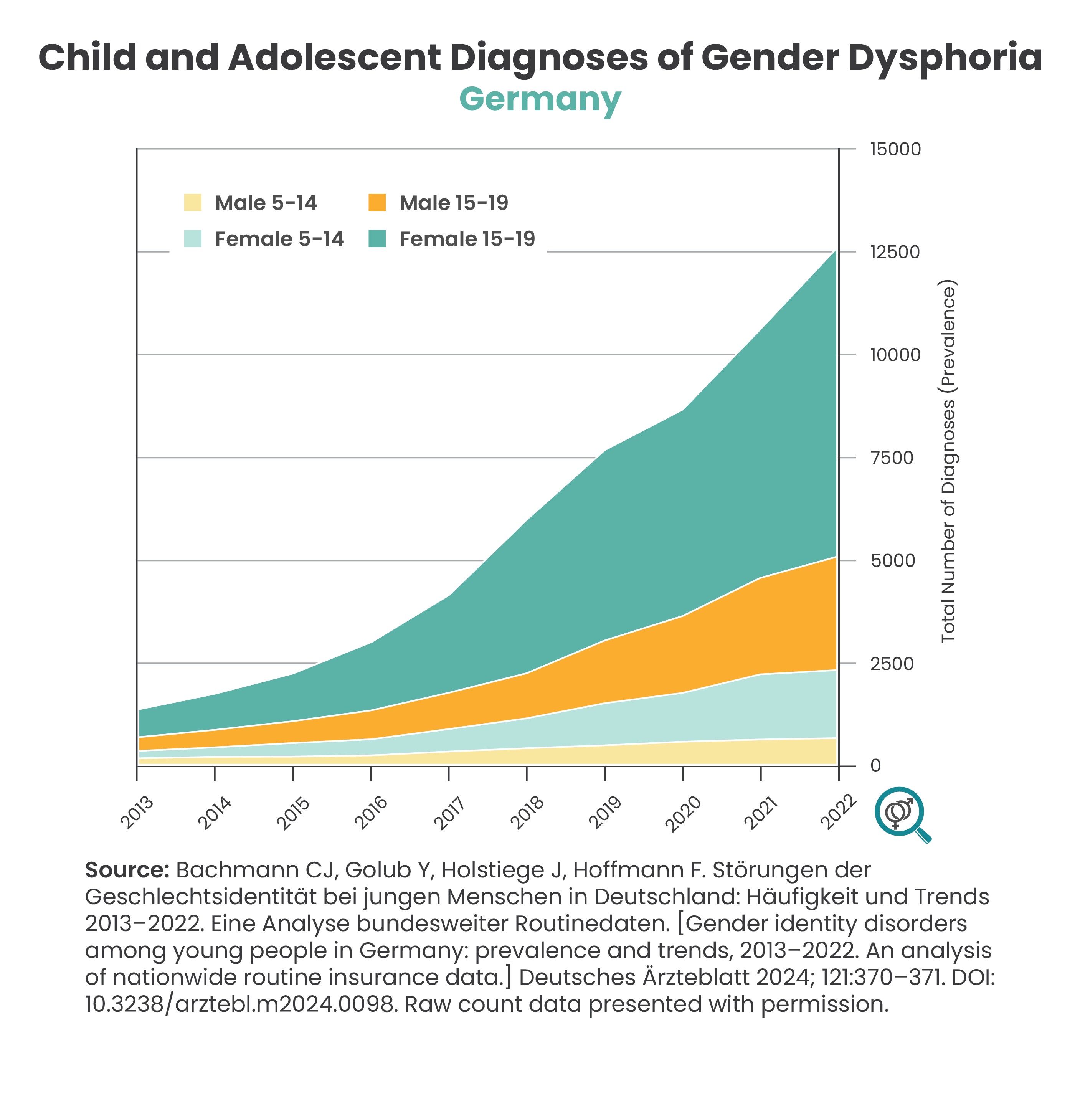
Sharp Increase in Incidence of Gender Dysphoria in Children and Young People
Historically, the small numbers of children presenting with gender dysphoria were primarily prepubescent males. In recent years, there has been a sharp increase in referrals of adolescents, and particularly adolescent females, to gender clinics. Many do not have a significant history of childhood gender dysphoria and a number suffer from comorbid mental health issues and neurodevelopmental conditions such as autism (ASD) and Attention-Deficit/Hyperactivity Disorder (ADHD). The reasons for these changes are understudied and remain poorly understood.
Childhood-onset gender dysphoria has been shown to have a high rate of natural resolution, with 61-98% of children reidentifying with their biological sex during puberty. The research into the course of gender dysphoria desistance among the cohort presenting with adolescent-onset gender dysphoria is still in its infancy, due to the novelty of this presentation. However, recent research from the UK clinic population suggests that 10-12% of youth may be detransitioning within 16 months to 5 years of initiating medical interventions, with an additional 20-22% discontinuing treatments for a range of reasons. The researchers noted that the detransition rate found in the recently-presenting population raises critical questions about the phenomenon of "overdiagnosis, overtreatment, or iatrogenic harm as found in other medical fields." U.S. data suggest that the rate of medical detransition has reached ~30%.



SEGM on Twitter
Treatment of Gender-Diverse Youth
Countries across the globe rethink pediatric gender transition
Historically, medical interventions to achieve the appearance of the desired sex were reserved primarily for adults with long histories of dysphoria. Such interventions were preceded by a prolonged engagement with the patient, including thorough psychological assessments. While objective population-level data of adult gender transitioners show persistent mental health struggles and sharply elevated mortality and morbidity, subjective patient-reported outcomes suggest low regret rates. Unfortunately, "regret" studies routinely fail to get in touch with 20-60% of the transitioned patients, leaving unanswered questions about the substantial number lost to follow-up. 'Regret" studies also suffer from other significant limitations. However, there is little reason to doubt that a number of adult transitioners, having made an informed decision regarding the balance of benefits, harms, and uncertainties, live rewarding lives.
However, around 2010's, there was a marked change in the approach to the management of gender dysphoria, particularly for gender-dysphoric youth. A number of countries in Western Europe, North America, and Australia, began to promote the "gender-affirmative" model of care for youth. Under this model of care, young people presenting with gender dysphoria or asserting a transgender identity are affirmed in their desire to undergo gender transition, and are provided with "barrier-free" hormonal and surgical interventions. While mental health professionals are often involved, their role is typically limited to preparing the young person for gender transition, regardless of any co-occurring mental health challenges or whether there was a relatively recent history of transgender identification. As such, the provision of medical intervention now happens with a much-reduced psychological assessment.
In the last 36 months, a growing number of Western countries have recognized the significant concerns with the "gender-affirmative" model of care, which became visible, in part, due to the growing voices of detransitioners and regretters coming from the novel population of gender-dysphoric youth. After completing systematic reviews of evidence, which showed that the risk-benefit ratio of youth transitions ranges from uncertain to unfavorable, these countries have begun to sunset the "gender-affirmation" practice in favor of an approach that favors psychosocial interventions as the first, and usually the only line of treatment available to most minors.
As of the current writing, the following countries have made sharp reversals of their previous "gender affirmation" practices or have signaled an intention to do so in the near future:
- Sweden has made the decision to no longer offer gender transition to minors outside of research settings, and restricted eligibility to the "classic" early childhood onset of gender dysphoria. All others are to be treated with psychosocial support and psychotherapy, with a focus on accepting and thriving in natal puberty.
- Finland has sharply restricted eligibility for gender transition to minors with a classic, early childhood-onset of gender dysphoria and no mental health comorbidities, and stated that psychotherapy should be the first line of treatment.
- England banned the use of puberty blockers for gender dysphoria outside of research trials. NHS England's interim clinical policy states that “The primary intervention for children and young people who are assessed as suitable for The Service is psychosocial (including) and psychological support and intervention; the psychoeducation main objective is to alleviate distress associated with gender incongruence and promote the individual’s global functioning and wellbeing.” On March 21, 2024, the NHS also updated its policy on cross-sex hormones for youth, removing the requirement of puberty blockers as a prerequisite step for cross-sex hormone treatment, presumably to make two policies better aligned (since puberty blockers will no longer be available). The final Cass Report was published in April 2024. SEGM's analysis concluded that the report signaled the end of the era of "gender-affirmative," gender-clinic-led model of care in England, with significant worldwide implications. No new prescriptions of cross-sex hormones for minors have been issued since the publication of the final Cass Report, and the use of puberty blockers are only be allowed as part of the PATHWAYS clinical trial, which is set to start recruitment during 2026.
- Following the Cass Report, Wales and Scotland joined England in stopping new prescriptions of puberty blockers as a treatment for gender dysphoria in youth <18. Scotland's policy goes even further than England's. While in England, cross-sex hormones can still be prescribed "around the patient's 16th birthday," they cannot cannot be accessed in Scotland until a patient is 18.
- Denmark has restricted eligibility for puberty blockers and cross-sex hormones, currently transitioning only 6% of youth referrals whose gender dysphoria is most consistent with the classic "Dutch" presentation (early childhood onset that intensified in adolescence, but otherwise uncomplicated by mental illness). This change in practice predated a change to treatment guidelines, which will be updated later this year.
- Norway's Healthcare Investigation Board (NHIB/UKOM) has deemed puberty blockers, cross-sex hormones & surgery for children & young people experimental, determining that the current “gender-affirmative” guidelines are not evidence-based and must be revised. Norway's public health authority has signaled an intention to respond to UKOM's concerns with an adjustment to the current treatment guidelines.
Other countries are seeing growing debate:
- In Australia, the Health Minister Mark Butler announced a national review of care and treatment guidelines for children and young people who identify as transgender. This announcement followed the decision by Queensland's Health Minister to initiate an independent review of prescribing puberty blockers and cross-sex hormones to gender-dysphoric youth, citing regulatory tightening in Finland, Norway, Denmark, Sweden, and the UK. The Queensland review was published in December 2025. The same day, the government of Queensland announced a pause in prescriptions of puberty blockers and cross-sex hormones for minors, pending the publication of the results from the UK's PATHWAYS study. Shortly after, the government of the Norther Territory announced restrictions for the prescription of puberty blockers.
- The Royal Australian and New Zealand College of Psychiatrists (RANZCP) acknowledged that "evidence and professional opinion is divided as to whether an affirmative approach should be taken in relation to treatment of transgender children or whether other approaches are more appropriate." New Zealand delayed its release of evidence review and recommendations for the use of puberty blockers, citing, in part, the Cass Report and the need to consider its findings and recommendations. On November 2025, the Health Ministry announced new regulation halting prescriptions of puberty blockers.
- Italy's National Bioethics Committee (CNB) just updated its stance on puberty blockers (PB) for gender dysphoria. The November 2024 guidance states that PBs should only be provided after mental health internvetions failed, and only in the context of proper research trials.
- The official journal of the German Medical Association published an article on the controversies in youth gender transition, stating that "the scientific evidence that these therapies are more beneficial than harmful is not as robust as has long been proclaimed." The article discussed the deficiencies in the evidence, noted that countries that were among the first to implement the practice of youth gender transition "are rowing back," and raised questions about implications for Germany's policy. A key German-language systematic review (with an English-translated appendix) updated the NICE systematic reviews and concurred with the findings concerning very low certainty of evidence. At the same time, the Association of the Scientific Medical Societies in Germany completed a "consensus" guideline that ignores the systematic reviews of evidence and promotes youth transitions. Following public criticism of the methodology, including by 15 prominent German Chairs of child adolescent psychiatry, the German guidelines were revised with considerably more cautious rec
- France's National Academy of Medicine has signaled that work is underway to address the emerging issues with medial "gender affirmation" in minors.
- Belgium's Director of Cochrane Belgium has expressed public concerns that puberty blockers are experimental and that the treatment guidelines promulgated by WPATH are not evidence-based. However, it is not clear whether the Belgium health authority plans to act on these concerns.
- In the Netherlands, Amsterdam UMC, the clinic that pioneered the Dutch Protocol, has responded to the Cass Report. The response indicated that the Dutch 2018 treatment guidelines are currently undergoing revision. According to the Dutch Health Council, "the Minister for Medical Care has asked the Health Council, among other things, to map out what is scientifically known about the (long-term) consequences of puberty blockers and gender-affirming hormone treatments for physical and mental health. The Minister also asks to compare the Dutch approach with the approach in other countries and with care standards and applicable laws and regulations." It is apparent that the international debate about youth transitions has reached the Netherlands.
In the meantime, in North America:
- At the Federal level, following the Biden administration's assertions that "gender-affirming" care is safe and effective, the Trump administration issued an executive order (EO) instructing federal agencies to stop the support for the hormonal and surgical gender transitions for minors, and to rescind their reliance on WPATH. The EO ordered the HHS to independently evaluate the evidence and approaches to youth gender dysphoria treatments within 90 days. This executive order will have significant implications for the practice of youth gender medicine in the United States.
- Florida was the first state to have its public health authority disallow medical transitions for youth under 18 (while "grandfathering" existing cases). At least 24 (and as many as 26) states passed laws to ban gender reassignment of minors, which have proven contentious. One of the state lawsuits, U.S. v Skrmetti, is currently awaiting the Supreme Court decision. (SEGM's submitted an Amicus Brief informing the courts of the issues at hand, available here).
- The Endocrine Society's (ES) President recently went on record asserting that gender transition of minors is a proven evidence-based practice. A letter from prominent clinicians involved in treatments of gender-dysphoric youth and evaluation of the outcomes sharply disagreed with such an assessment and called for the medical societies to "align their recommendations with the best available evidence—rather than exaggerating the benefits and minimizing the risks." The ES is currently in the process of updating its treatment guidelines, with no estimate for when n
- Most recently, the American Academy of Pediatrics (AAP) finally conceded it was time to conduct an independent review of the evidence and update its guidance, but it has already presaged the review's conclusion, which is that it will support the current pro-affirmation AAP position. This contradicts findings of multiple systematic reviews of evidence that found the benefits of gender transition for minors are highly uncertain, while the risks may be significant. Specifically, if the Endocrine Society's treatment guidelines for gender-dysphoric youth are followed, a minor's future sterility is likely. Other health risks include compromised bone health, altered brain development, cardiovascular complications, and a number of other, as yet unknown, risks.
The Dutch Protocol
The practice of medically transitioning minors, currently referred to as "gender-affirmative care," began to gain momentum following a single-site study in the Netherlands. Previously, gender transition was available only to mature adults, with the average age of transition frequently in the 30's. However, it was noted that the results of adult transitions were frequently disappointing, which was believed to be explained by unsatisfactory cosmetic outcomes, particularly for males, who had a "never disappearing masculine appearance." in the 1990's, the Dutch clinicians began to experiment with transitioning minors using endocrine interventions with the hope that a better cosmetic outcome would also lead to better mental health ones. The results of the innovative Dutch experiment, which has become known as "the Dutch Protocol," were documented in two publications: the 2011 study, which reported on cases who underwent puberty blockade, and the 2014 study, which reported on a subset of the cases who completed surgeries, including the removal of ovaries and testes upon reaching the age of 18.
The youth in the Dutch study reported high levels psychological functioning at 1.5 years after surgery, the study end point. However, both of the studies suffer from a high risk of bias due to their study design and suffer from limited applicability to the populations of adolescents presenting today According to a recently-published overview of the Dutch protocol, the interventions described in the study are currently being applied in the way there were not intended. Specifically, adolescents who were not cross-gender identified prior to puberty, who have significant mental health problems, as well as those who have non-binary identities are now commonly treated using endocrine and surgical interventions described by the Dutch—yet all of these presentations were explicitly disqualified from the Dutch protocol.
The study itself suffers from significant limitations, ranging from a weak study design, only marginal improvements in psychological function, and number of under-reported adverse health events that occurred over the course of they study (including 1 case of death and 3 cases of severe morbidity). Researchers have also questions the validity of the gender dysphoria resolution reported by the Dutch, in light of their unusual handling of the gender dysphoria scale. Despite these limitations, the Dutch clinical experiment has become the basis for the practice of medical transition of minors worldwide and serves as the basis for the recommendations outlined in the 2017 Endocrine Society guidelines and has given rise to the so-called "gender affirmative" model of care for youth, which requires access to puberty blockers, hormones, and potentially surgery.
The medical pathway of the Gender-
Affirmative model consisting of...
- Puberty blockers (GnRHas)
- Lifelong cross-sex-hormones
- Mastectomy or breast implants
- Removal of ovaries or testes
- Hysterectomy
- Surgical removal and revision of sex organs
Hormonal & surgical interventions
can lead to:
- Irreversible physical changes
- Medical complications/ drug side effects
- Surgical complications
- Infertility
- Arrest of a normal developmental process (puberty)
Multiple studies have found associations:
- Bone/skeletal impairments
- Cardiovascular complications
- Premature death
- High rates of post-surgery suicide
...is based on a single Dutch study:
- 55 subjects (only 40 with complete data)
- 100% had childhood-onset gender dysphoria (no adolescent-onset gender dysphoria cases)
- Only 1.5 year post-surgery follow-up at an average age of under 21
- No control group
- No physical health effects evaluation
- One adolescent died as a result of post-operative complications. Several others could not pursue treatment due to new health issues arising following hormonal administration
- Unchanged or worsening gender dysphoria and body image difficulties while on puberty blockers, especially among natal adolescent females
Despite the uncertainties and poor evidence, hormonal and surgical interventions are being scaled up. They go beyond the experimental “Dutch protocol” by:
- Encouraging early social transition, explicitly discouraged by the Dutch protocol
- Being applied to young people with adolescent-onset gender dysphoria, a population not included in the Dutch study
We agree with the concerns voiced by the recent publication, "Reconsidering Informed Consent for Trans-Identified Children, Adolescents, and Young Adults," that the Dutch studies have been misunderstood and misrepresented as providing evidence of the safety and efficacy of hormonal and surgical "gender-affirming" interventions for all youth. It is important that both the strengths and the weaknesses of these studies are thoroughly understood, as these two studies represent the best available evidence behind the practice of pediatric gender transition. You can read more about the strengths and limitations of the Dutch studies here.
Need for Caution and Better Research
The history of medicine has many examples in which the well-meaning pursuit of short-term relief of symptoms has led to devastating long-term results; for example the past use of thalidomide, lobotomies, and the recent opioid epidemic. The "gender affirmative" model commits young people to lifelong medical treatment with minimal attention to the etiology of their conditions, and the psychosocial factors contributing to gender dysphoria. This model dismisses the question of whether psychological therapy might help to relieve or resolve gender dysphoria and provides interventions without an adequate examination.
We are asking clinicians and researchers to halt this uncontrolled experimentation on youth and replace it with a supportive framework of research that generates useful evidence about the etiology of gender dysphoria and the benefits and harms of various interventions. We need to know:
Which factors contribute to the development of gender dysphoria?
Which are the most effective interventions in gender dysphoria?
What are the long-term outcomes of those interventions?
Support Our Work
SEGM promotes safe, compassionate, ethical, and evidence-informed healthcare for children, adolescents, and young adults with gender dysphoria. We are working on a range of projects—from evidence evaluation, to supporting new and ongoing research, to enabling scientific collaborations between hundreds of clinicians and researchers worldwide.
To support our work, please consider making a contribution.
Alternatively, you can donate by mail:
Society for Evidence-Based Gender Medicine
148 Blue Lakes Blvd N #361
Twin Falls ID 83301
SEGM is a registered 501(c)(3) nonprofit organization. Contributions to SEGM are tax-deductible to the extent permitted by law. SEGM's tax identification number is 84-4520593.