Update: On January 15, 2024 the World Health Organization (WHO) issued a new announcement, extending the public comment deadline regarding its planned "trans and gender diverse" guidelines to February 2, 2024. SEGM will be analyzing the new WHO announcement and the FAQs that accompany it. In the meantime, these appear to be the key takeaways:
1. The WHO transgender/gender diverse guideline will address treatments of adults exclusively, and will not issue recommendations for children or adolescents. WHO stated that due to uncertain evidence for "affirming care" for children and adolescents, it will focus its recommendations on adults only. WHO's January 15, 2024 acknowledgement that "the evidence base for children and adolescents is limited and variable regarding the longer-term outcomes of gender affirming care for children and adolescents" is noteworthy. However, this language does indicate that WHO currently believes that the evidence for the vulnerable cohort of young adults aged 18-25 supports the stated plan to recommend an expanded access to hormones for this group.
2. The guideline panel composition (GDG) may undergo further changes. One of the more controversial GDG members no longer appears in the group "due to scheduling conflicts." While the rest of the GDG composition remains unchanged, the announcement suggest that the group composition is not complete and that additional changes may be made: "Following the completion of the extended public feedback period, the final list of GDG members is expected to be announced... ."
3. The timeline for the guideline development process appears to have been extended. The originally-announced February 2024 meeting may still take place (it is not addressed in the announcement), but the process is now described as the beginning of the work which may take "up to 2 years." The original announcement stated that the February meeting of the GDG would be to "formulate recommendations" and "suggest implementation considerations"—the steps that signal the end, rather than the beginning, of the guideline development process.
We will share more details as we complete our analysis of the latest WHO announcements.
Below is our original post in response to the December 18, 2023 announcement:
On December 18, 2023, the World Health Organization (WHO) announced the final composition of the Guideline Development Group (GDG), tasked with developing guidelines related to transgender health in 2024, and sought public comment. The guidelines will focus on 5 areas: provision of gender-affirming care, medical training, gender-affirmative health policies, “provision of health care for trans and gender diverse people who suffered interpersonal violence based in their needs”, as well as “legal recognition of self-determined gender identity.” The group is scheduled to meet at the WHO headquarters in Geneva on February 19-21, 2024 to evaluate and interpret the evidence, formulate guideline recommendations, and suggest implementation strategies. Since adolescents and young adults are the largest and fastest-growing group of transgender-identified individuals, it is likely that the WHO guidelines will apply to this vulnerable group as a target population. 1
There are several concerns related to this WHO announcement. Specifically, they include a biased guideline panel composition, an inappropriately handled public comment period, and the rushed guideline development process overall. Further, the language of the announcement does not appear to be neutral. It states the goal of "increasing access and utilization" of, presumably, gender-affirmative interventions by "trans and gender diverse people," and declares the goal of legal recognition of "self-determined gender identity." This suggests that the decision to promote gender transition in the respective societal arenas (medical, policy, legal) has already been made before the group has even met to review and interpret the evidence—a step that must both precede and inform the guideline recommendations. All these concerns put this WHO guideline at risk of producing biased and untrustworthy recommendations.
Countries with strong public health authorities who have demonstrated a commitment to the principles of evidence-based medicine in the area of youth gender medicine (e.g., England, Sweden, Finland) are likely to ignore biased WHO guidelines. However, countries with fewer resources, or countries where public health authorities are just starting to note the international debates, will bear the brunt of contending with a WHO-endorsed guideline that may have the appearance of an evidence-based guideline, but which may be promoting potentially non-beneficial or even harmful interventions for gender-dysphoric youth. For this reason, individuals and organizations concerned with the health and well-being of gender-dysphoric youth should pay close attention to the WHO announcement, and the significant concerns it raises. We elaborate on each of these concerns below. The deadline for public comment is January 8, 2024.
Biased guideline panel composition
Guideline panel composition (i.e., the GDG membership) is crucial to ensure a methodologically appropriate, evidence-based guideline development process. According to the WHO guideline development handbook, a conflict of interest (COI) is “a set or circumstances that creates a risk that professional judgment or actions regarding a primary interest will be unduly influenced by a secondary interest.” The handbook distinguishes between two types of COIs, financial and nonfinancial. The latter are most relevant to these guidelines. They are described as “any interest that could be reasonably perceived to affect an individual’s objectivity and independence while working with WHO.” Of note, this is also the definition that WHO describes they provide to potential GDG members when asking them to declare such conflicts. There is special mention of a subtype of nonfinancial COI, “intellectual conflict of interest,” defined as “academic activities that create the potential for an attachment to a specific point of view that could unduly affect an individual’s judgment about a specific recommendation”.
According to section 6.6 of the handbook, nonfinancial COIs that must be identified and appropriately managed include the following:

Unfortunately, even a cursory review of the GDG membership shows that a number of members in the group have significant COIs in one, two, or all three areas: prior publication that may comprise the evidence base under consideration; public declaration of a firm opinion or position related to the subject matter; and affiliation with organizations related to the subject of the guidelines. Further, even a cursory review of the GDG membership shows that many have a strong intellectual bias in favor of “gender affirmation.” More than 1/3 are members of WPATH (some senior leaders), which promotes medical gender-affirmative approaches. Further, several have expressed strong opinions (in research and legal settings) that a transgender identity has an immutable biological basis; asserted that gender-affirming interventions are always safe and effective and never harmful; and stigmatized non-invasive alternatives such as exploratory psychotherapy as "conversion therapy."
Below are some quotations from the GDG group members that demonstrate the direction and strength of the views of several GDG group members:
"Research indicates that immutable biological and genetic factors influence a person’s gender identity... [it] is wrong to imply that a transgender person’s gender identity is ... less intrinsic or less important than their sex assigned at birth, or that it stands in contrast to 'biological reality.'” Position expressed in 2019 in a legal setting by GDG member Walter Bockting, past president of WPATH overseeing the WPATH launch of "Standards of Care 7" and former editor of the official WPATH journal.
“The actual side effects of gender affirming medical care, for those who can access it, include a significantly improved quality of life, significantly better health and wellbeing outcomes, a dramatic decrease in distress, depression and anxiety and a substantial increase of gender euphoria and trans joy... We are not at risk of harm by affirming our gender." Position expressed in 2022 by Teddy Cook, Vice-President of AUSPATH in a media interview.
“So-called “gender-exploratory therapy” is essentially indistinguishable from conversion practices. Pass the word along.” Position expressed in a Tweet in 2023 by Florence Ashley, a Canadian transfeminine law professor promoting their publication.
Of note, the above positions are not supported by the evidence, and as such, they represent opinions not facts. For example, the view that exploration of one's gender distress is "conversion therapy" is at odds with the current recommendations by Sweden's, Finland's, and England's health authorities that non-invasive psychosocial interventions should be the first line of treatment for gender dysphoric youth. Further, no quality systematic review of evidence and no quality long-term study has been able to identify credible benefits of gender transition to mental or physical health. Additionally, no study to date has been able to identify an immutable biological factor leading to a transgender identity—a fact acknowledged by the Endocrine Society's scientific statement on sex and gender identity.
In addition, the group's composition is unbalanced: there is a marked absence of individuals who believe that the harm-benefit ratio of gender transition is unfavorable for many of the young people currently wishing to undergo gender transition. This view is now expressed not only by a growing number of detransitioners (one study estimates medical discontinuation rate of 30% within 4 years of starting hormones), but also by a number of progressive public health authorities and professionals who have participated in the turns toward caution in Sweden, Finland, England, Norway, Denmark, France, and other countries.
This biased panel composition where the majority of the GDG group have expressed one-sided strong opinions on the subject matter appears to be in contradiction of WHO’s own conflict of interest management policies. The WHO handbook for guideline development dedicates a full chapter to the issue of conflicts of interest (COI) management, which states that "management of conflicts of interest is essential to the development of unbiased and credible recommendations.”
The reason why COI management is so critical is because the guideline panel (GDG) is responsible for all the critical aspect of the guideline development, each of which requires subjective judgement. According to the WHO handbook, the guideline panel (GDG) plays the following role:
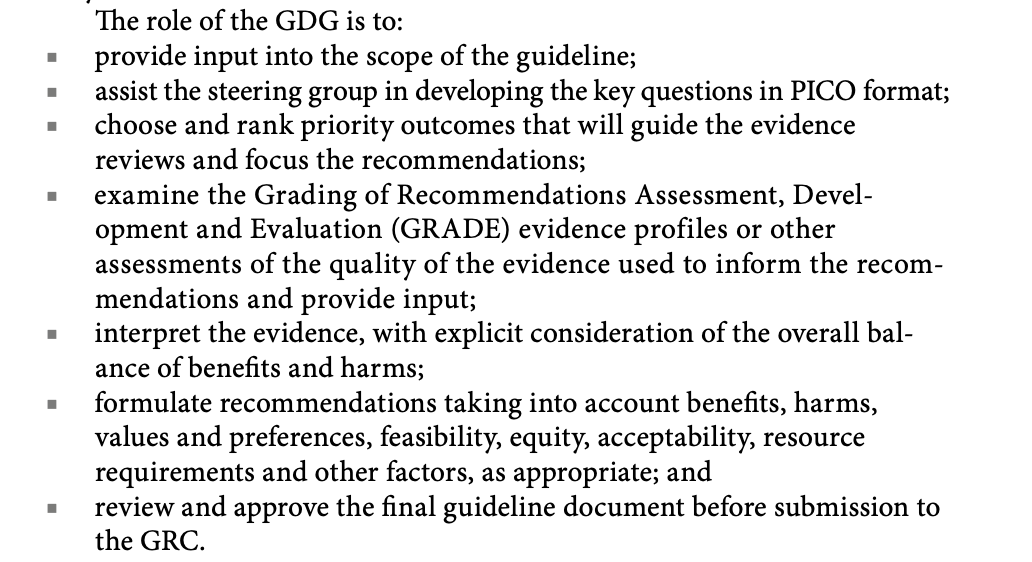
Many of the tasks described above require making value judgments. For example, the guideline panel must decide which outcomes are critical and important; determine whether magnitude of the benefits and harms on those outcomes is important; and determine how to balance benefits and harms.
Because panels make so many value judgments when developing recommendations, management of conflicts of interest (COI) is crucial. The WHO handbook describes a process for management of COI for GDG members. The process starts with the collection and declaration, and if a relevant and significant COI exists, that may result in high risk of bias or decreased credibility, the GDG member is not appointed. If the COI exists but is not expected to result in high risk of bias or decreased credibility, the COI is managed by restricting participation (Figure 6.1 in the handbook).

In addition to the lack of diversity of views, the GDG composition is notably missing methodologists skilled in evidence synthesis and guideline development.
The strong pro-transition views held by the GDG members, a marked absence of any individuals or professionals who are concerned about the unfavorable harm-benefit profile of youth gender transition, and a lack of independent methodological expertise among the current guideline panel (GDG) members put the eventual guideline recommendations at high risk of bias and seriously diminishes credibility of the recommendations.
Inappropriately handled public consultation
The timing of the public comment period (announced on December 18th, over Christmas and New Year’s holidays, with a deadline to comment on January 8th) is far too short for the interested individuals, organizations, and other stakeholders to take note of the announcement, engage with the panel composition, and comment on it. Of note, when the original announcement of this effort was made earlier this year (which contained only a partial list of the GDG members), it also occurred during a common summer holiday period and provided a scant 2-week comment period and an incomplete panel list.
Further, the fact that WHO already announced the February 19-21, 2024, date for the group’s meeting in Geneva to make its recommendations suggests that WHO is not anticipating any meaningful panel composition changes in response to the public consultation.
An unusually rushed process for creating a key guideline
Guideline development is a lengthy process in any organization—and especially WHO. It involves many steps, from panel formation, commissioning evidence synthesis from independent groups through an involved and lengthy request for proposal processes, to engaging independent methodologists to support the development of the guideline.
The fact that the first time the complete GDG composition was announced on December 18, 2023 (the prior June 2023 announcement only listed 2/3 of the panel members), and the group’s meeting to make recommendations is already scheduled for February 2024, signals an extremely rapid, and even unprecedented, guideline development speed. The guidelines’ wide scope—encompassing medical, policy, and legal considerations—makes it even less plausible that a rushed process can ensure that biases in the final recommendations are minimized so that the recommendations may be viewed as credible.
SEGM Recommendations
Given the profound problems above, it is advisable that WHO pause the process (including the postponement of the February 2024 Geneva meeting), and go back to the drawing board. SEGM has the following recommendations:
- WHO must ensure that the guideline panel (GDG) properly represents the diversity of views on this complex matter. There is a clear divergence in approaches to the management of gender dysphoria with regard to the provision of hormonal interventions for youth, which has become much more apparent in the last 36 months. Current approaches range from “gender-affirmative” (providing all youth who desire body modification all the medical technologies available to deliver the desired physical changes), to psychotherapy-led with medical interventions only as last resort for a narrowly defined population of youth, to moratoriums until clinical research can demonstrate the safety and efficacy of any intervention. The GDG composition must represent this diversity of views.
Further, the medical guidelines must address the growing phenomenon of detransition—a vulnerable group of patients for whom no organization has created any clinical practice guidelines. For this reason, detransitioners and professionals working with this patient group must be represented.
When properly represented, the divergence of viewpoints and the strengths of many of
the views, will make it hard or impossible to achieve consensus on the balance between desirable and undesirable consequences when comparing the different options for the management of these individuals, which is crucial for the development of each recommendation. For this reason, it is strongly recommended that WHO engage an independent methodologist to lead this guideline development process, ensuring the methodologist’s key role at each stage, directing evidence synthesis and evaluation, ensuring that no single group’s values and preferences unduly influence the harm-benefit ratio and preparation of the final recommendations. - WHO must ensure that conflicts of interest are properly managed. Given the challenge of the GDG members; completely and accurately reporting their conflicts of interest (especially those in “intellectual” category), WHO should utilize a well-known strategy for circumventing this problem by appointing a steering committee to search for information about the prospective members (a search of relevant websites or academic profiles) in order to determine whether there may be anything they failed to declare. The steering committee should then judge the severity of any COIs and develop a mitigation strategy.
Because the assessment is subjective, it important that the steering committee members are independent and have not taken a point of view on this contentious subject. An extended public consultation period will ensure that members of the public can identify and flag any concerns so that all COIs are mitigated.
- WHO must ensure transparent reporting of the guideline development process. The Steering Committee and the WHO Guideline Review Committee must ensure a transparent reporting related to all key stages of the guideline development process. In particular, in addition to adhering to the highest methodological standards when deciding on the strength of recommendations, WHO must specify the value judgments made during the interpretation of the evidence and development of the recommendations.
Value judgements become especially important when the body of evidence is of very low and low certainty—as has been found by every quality systematic review of evidence for treatments of gender dysphoria to date. As with any controversial topic, the guideline should explicitly and transparently report whose values are prioritized and why these priorities are appropriate; which thresholds the GDG used to determine the magnitude of the effects (and where these measures were obtained), and why some factors affecting the recommendation are given more weight than others.
SEGM looks forward to submitting this feedback to WHO ahead of the stated deadline on January 8th, 2024 by emailing our concerns to [email protected]2
Footnotes:
1. According to a recent article published in the BMJ, WHO subsequently clarified that its recommendations will focus only on adults. However, the original official WHO announcement did not contain this information, and it has not been updated with this clarification.
2. SEGM submitted a comment and a set of questions for WHO on behalf of over 100 clinicians and researchers from 18 countries. As of January 13, 2023, we have not yet received a reply.
Supplementary information
- January 15, 2024 announcement which clarifies the process
- The new announcement
- New FAQs
- Updated guideline development group (GDG) list (one member is no longer part of the group)
- December 18, 2023 announcement with complete GDG composition
- June 28, 2023 original announcement of WHO's intention to produce transgender guidelines, with a partial list of GDG members.
- WHO groups sponsoring the transgender guidelines:
- Departments of Gender, Rights and Equity - Diversity, Equity, and Inclusion (GRE-DEI)
- Global HIV
- Hepatitis and Sexually Transmitted Infections Programmes (HHS)
- Sexual and Reproductive Health and Research (SRH)
- First mention of the plans for the guideline:
- Link to the WHO guideline development book: