Denmark Joins the List of Countries That Have Sharply Restricted Youth Gender Transitions
A major medical journal Ugeskrift for Læger, the Journal of the Danish Medical Association, confirmed that there has been a marked shift in the country’s approach to caring for youth with gender dysphoria. Most youth referred to the centralized gender clinic no longer get a prescription for puberty blockers, hormones or surgery—instead they receive therapeutic counseling and support.
In the course of less than a decade, like every other Western country, Denmark experienced an exponential increase in the number of young people presenting with gender dysphoria. In 2014, there were only 4 documented pediatric cases who requested gender reassignment. By 2022, the number of referrals grew by 8700% to 352, similar to the several-thousand-percent increase in less than a decade witnessed by a number of Western countries. As the number of young people wishing to undergo gender reassignment increased, so did the rates at which Danish gender clinicians transitioned them. By 2018, Denmark's centralized gender service was medically transitioning 65% of referred youth. This was similar to the proportion of referred children who got transitioned reported by other pediatric gender clinics. For purposes of comparison, the Netherland’s Amsterdam gender clinic reports transitioning 73% of late-onset referrals and 85% of early-onset referrals and in the US, researchers analyzing data from Seattle Children’s Hospital gender clinic reported that over 60% of the referrals underwent medical transition with puberty blockers or cross-sex hormones within one year of intake.
However, following systematic reviews of evidence conducted in Europe and the subsequent reversal of the “gender-affirmation” paradigm in favor of a cautious, developmentally-informed approach that prioritizes psychosocial support and noninvasive resolution of gender distress in Sweden and Finland, Denmark appears to have made a quiet but resolute shift to treat most youth presenting with gender dysphoria with supportive counseling rather than puberty blockers, hormones, or surgery. In 2022, only 6% of those referred to Denmark’s centralized gender clinic were prescribed endocrine interventions (puberty blockers and/or cross-sex hormones).*
The rationale for this shift was explained in a recent publication in Ugeskrift for Læger (“Weekly Journal for Physicians”), the Journal of the Danish Medical Association. This Danish-language article provides one of the most sober discussions to date of the inherent medical and ethical uncertainties of providing minors with profound, life-altering interventions in the context of very limited understanding of the epidemiological shift in the population presenting for care, the growing rates of detransition, and the profound uncertainty about long-term outcomes.
The authors can hardly be accused of being “armchair critics.” They are the very clinicians responsible for assessing youth and approving them for gender transitions in Denmark. Realizing that their well-meaning intentions were based on insufficient evidence, and seeing the growing evidence of harm, they sharply reversed course. Today, only 6% of the referrals are approved for hormonal transition, and no minors are allowed to transition surgically.
The article is open-access, and only available in Danish. Below, we provide a synopsis.
- The Danish centralized pediatric gender service was launched in 2016. Denmark opened a centralized gender transition service for minors in 2016, using a multidisciplinary approach that encompasses intake, evaluation, consultation, and referrals for puberty blockers and cross-sex hormones.
- The rationale for launching the pediatric gender transition service was the Dutch studies’ reported success. The Danish youth gender transition service was launched based on the experience of the Amsterdam gender clinic and reports of its positive outcomes “suggesting that early hormone therapy resulted in better psychological and physical outcomes and less need for surgery in adulthood” as well as “body satisfaction, low rates of regret, and few side effects.” The two studies supporting this premise were the Dutch protocol as described by the Dutch clinicians in 2012, and the famous 2014 “Dutch study.”
- A key assumption, now in question, was the permanence of transgender identity in youth with longstanding gender dysphoria that intensified in puberty. According to the authors, the Dutch “trials” of gender transition were justified insofar as it was believed that a cross-sex identity in adolescents with longstanding gender dysphoria that intensified in adolescence would be permanent, or “stable.” However, the authors now concede that there are significant questions brought about the growing rate of detransition, and concerns “about the generalizability of these studies,” especially their applicability to the young people referred to gender clinics today.
- The significant “underexplained” increase in referrals of adolescents over age 11 “mainly made up of birth-assigned girls” became a major red flag. The authors describe a profound change in the epidemiology of gender dysphoria in youth following the launch of the centralized pediatric gender clinic service. “In Denmark, the number of referred persons has increased from 97 in 2016 to 352 in 2022, of which birth-assigned girls aged 11-18 make up 70%”. Noting the “excess of birth-assigned girls” among gender dysphoric youth, the authors express concern that “the background for the change is underexplained.”
- Another red flag is the high rate of psychiatric comorbidities in currently-presenting cases. The authors note that unlike the Netherlands, where gender dysphoric youth reportedly have a relatively low rate of psychiatric comorbidities (33%), in Denmark and other countries there is a much greater proportion of gender dysphoric youth with comorbid mental illness (e.g., 75% in Finland). These conditions include depression, anxiety, suicidal thoughts/self-harm, autism spectrum disorder (ASD) and attention deficit hyperactivity disorder (ADHD).
- The authors raise a new concern: gender dysphoric youth have a younger age of pubertal onset. They reference a Danish study that found earlier puberty in youth with gender dysphoria compared to the general population of adolescents. They do not elaborate on the implications of this finding, but note that overall the pubertal age has been declining.
- The authors call out more generally the growing rates of gender nonconformity in youth, and especially females, independent of the youths’ wish to medicalize. The study authors cite the results of the Danish Project SEXUS study which found a sharp increase in gender nonconformity (21.2% of females and 15.7% of males ages 15–24 years). The authors note a generally “higher incidence of non-gender-normative behavior among girls” and “low tolerance for non-gender-normative behavior in boys.”
- The authors explicitly identify “social influence” as a contributor to the concerning epidemiological shift in gender dysphoria presentation. The idea that teens are products of their social environments and can adopt transgender identities following social influence does not appear to be controversial in Denmark. The authors openly discuss the possibility of social influence as directly contributing to the rapid rise of post-pubertal onset of gender dysphoria in youth. They also opine that the availability of treatment itself may have contributed to rapid rise of trans-identification in youth.
- The Danish clinicians are concerned by growing rates of detransition among those who initiated transition in youth and a lack of research into the detransition phenomenon. “In recent years, there have been reports of reversal of hormone-induced permanent changes to the body that began in youth. There are no systematic estimates of the frequency or reasons why hormone treatment is discontinued.”
- The Danish clinicians are now concerned that the basis for gender-transition of large numbers of minors with diverse presentations of gender dysphoria is a single short-term Dutch study based in a different population and which has failed replication outside the Netherlands. Throughout the article, the Danish clinicians describe their initially positive view of the Dutch research, and their now growing concern about the lack of applicability of the Dutch experience from years past to the current clinical realities in the rest of the Western world. They appear to be signaling a widening gap between the positive trends that the Dutch clinicians continue to report (youth with low rates of mental illness, low rates of detransition, and positive short-term transition outcomes), and the problems emerging in the rest of the Western world (much higher rates of comorbid mental illness, an inability to show robust and reliable improvements in mental health, and growing rates of detransition).
- International changes, and especially those in the Nordic European countries, appear to have directly influenced Demarks’ move to a more cautious approach. In Finland and Sweden, youth with post-puberal onset of gender dysphoria are not typically considered to be candidates for medical transition in adolescence. Denmark’s gender clinicians quoted these changes in their new move to base treatment eligibility in part on the “duration” of gender dysphoria.
- As a result of the above-mentioned concerns and international changes, Denmark has sharply restricted eligibility for hormone interventions for youth. The authors state that Denmark has “adopted a more cautious approach to hormone therapy until more evidence of its beneficial effects is available.” While the article does not provide year-over-year referral-to-treated ratios, another source confirms that in 2018, two-thirds (65%) of referred youth were transitioned and by 2022 this percentage fell to 6% (22/352).
- The authors conclude with a call for more research and international collaboration:
"Several countries, including Denmark, have adopted a more cautious approach to hormone therapy until more evidence of its beneficial effects is available [2, 17]. In particular, there is a lack of knowledge about the increasing proportion of young people with onset of gender-related discomfort after puberty [2, 17, 23] and the presumably increasing proportion with mental disorders, as new studies suggest that the positive effects are not replicated in this group [22, 29]. There is a need for healthcare services that can be flexibly adapted in the future and systematic international cooperation in research and exchange of experience."
The current Danish treatment guidelines were published in 2018 and are due to be updated later this year. While the specifics of the changes have not yet been made public, the new approach described in the article foreshadows the likely principles and practices that will be included in the updated guidelines, specifically:
- Thorough psychological assessments are required to determine whether gender dysphoria is related to a mental health disorder such as ASD, or psychosis. All young people are to be thoroughly assessed using broad and lengthy diagnostic interviews with multiple reporters including schools and parents as well as cognitive testing. The assessment aims to determine whether gender discomfort may be an aspect of a psychiatric disorder or mental illness.
- Minors whose gender dysphoria differs from the classic “Dutch” definition (i.e., early onset of gender dysphoria that worsens after puberty, no significant mental health comorbidities) will only be offered psychosocial, supportive treatment. The centralized team will assess for the appropriateness of medical transition. Most presenting cases are rejected from consideration for medical transition and instead are referred to “support or advisory conversations.” Of note, while the authors reference the longstanding duration of gender-related distress that worsens in puberty they do not explicitly require early childhood onset of gender dysphoria. It remains to be seen how explicit this requirement is in the updated guidelines.
- Not every otherwise eligible minor will be considered able to consent. The authors explain that“…the level of functioning, stability and how any psychopathology, cognitive level and psychosocial conditions affect identity development and the ability to reflect on and make decisions about gender reassignment treatment.”
- Teens ages 15 and older retain the right to consent to treatment without parental agreement or consent, but the treatments offered will prioritize counseling. According to the current 2018 Danish treatment guidelines, when a 15-year-old minor and their parents disagree about gender transition, the minor can proceed without parental consent. This is because Denmark’s laws consider 15-year-olds competent to make medical decisions. While these laws will not change, the authors recognize the important role of parents in this unusual situation, and underscore that the treatments offered to the teens will be “psychosocial support for the young person” and they further assert that “ideally all decisions are made in consultation with the parents.”
- For the remaining few cases that will qualify for transition, significant uncertainties are explicitly identified. Irreversible changes are called out, along with the health risks: “…both types of sex hormones cause reduced fertility, however the degree and reversibility of this remains unknown. Contraindications to hormone therapy are abuse, suicidal ideation/self-harm, severe psychological distress and worrisome somatic conditions (eg cancer, thromboembolic disease).” It is acknowledged that hormone treatment will be lifelong.
- Surgical interventions in minors, already rare, will likely be removed as an option. The current treatment guidelines do not allow genital surgeries for those under 18, but it appears that mastectomies for some older teens are still an option (although perhaps an option on paper only). Recent comments by the Danish Minister of Health suggest that mastectomies may be officially disallowed in the updated guidelines.
“I can also inform you that the National Board of Health [“Sundhedsstyrelsen”] issued a new guideline for gender reassignment surgery on March 28 this year at the latest, which is now in consultation. In the new referral guidelines, it is no longer possible to offer surgical treatment to children under the age of 18... An option that, by the way, has never been used in Denmark.” **
SEGM Take-Away
In the last several weeks, health journalists have reported that change may be afoot in Denmark. The article in Denmark’s Medical Association journal Ugeskrift for Læger leaves very little doubt that Denmark too has made a course correction in youth gender transitions, restricting this option to very few cases, while prioritizing counseling for the vast majority of the currently presenting youths. The article is an excellent summary of the rise-and-fall-of the “gender affirmation” model of care in Denmark. It describes how in 2016, following the influence of other northern European countries, Denmark chose to offer “a treatment approach with few barriers to hormone treatment for children and young people with gender dysphoria.” The treatment was justified by the foundational Dutch studies, “which indicated better well-being and body satisfaction after hormone treatment, a low degree of regret and few side effects.” However, the increasing number of referrals, changes in the presentation in gender dysphoria, and growing reports of regret—combined with a lack of long-term outcomes of the one and only sample of youth (n=55) on which the entire practice of gender transition rests—led the Danish clinicians to reverse course.
This change is notable. In 2014, Denmark became the first European country to pass a “self-id” law for adults whereby adults did not need a diagnosis of gender dysphoria to register a legal sex change. Denmark continued to be a leader in destigmatizing transgender identities and in 2017, becoming the first country in the world to remove “Gender Identity Disorder” (DF64) from the its public health authority's list of mental illnesses. To provide treatment, healthcare practitioners were instructed to use a “Z” code, “contact due to gender identity” (DX78X)." The barrier-free transition of minors, launched in 2016, was the logical next step.
To fully appreciate the scope of the changes underway in the treatment approaches for minors, it is helpful to review Denmark’s 2018 official practice guidance, Health professional help with gender identity issues (English-language version here). The guidance does not preclude any presentation of gender dysphoria from eligibility for transition; there is no minimum age for transition; and at age 15 minors who are considered able to understand the consequences of treatment for gender dysphoria may obtain medical transition services without parental consent.
Recently, Danish Minister of Health Sophie Løhde acknowledged that country’s national pediatric center for gender dysphoria in Copenhagen has grown “reluctant to offer hormone treatment compared to before,” particularly to youth with post-pubertal onset of gender dysphoria. The Danish Health Minister praised this change in practice, noting that “it is a positive thing that there is a response to research and experience... both in Denmark, but also abroad, which we must follow closely. And this knowledge and experience lead to adjustments in the current treatment options.”
While countries in Europe are increasingly leaning on one another’s experience and collective knowledge to devise an approach to intake, screening, and support of gender-dysphoric youth in order to safeguard them from inappropriate, non-evidence-based gender reassignment practices, the American medical establishment continues to double-down and “do it alone.” Earlier this month, the American Academy of Pediatrics (AAP) finally conceded to conduct an independent review of the evidence and update its guidance. This decision has come several years too late: the first call for these actions came from AAP members in 2019 and has been repeated every year since.
However, at the same time, at its 2023 Annual Leadership Forum earlier this month, AAP paradoxically reaffirmed its current “transition for all those who want it” affirmative care approach, refusing to acknowledge or consider the problems that have been documented by the recent European systematic reviews and react in real time. Rather than working collaboratively, as the Danish clinicians have suggested in their article, the CEO of the AAP has described a decidedly American-exceptionalism approach: “they engaged in their process, we’re engaging in our process.” And just earlier this week, the official AAP website platformed another article promoting gender transition of minors by two gender clinicians who reassured America’s pediatricians that "affirmation" is beneficial while caution is harmful: “When pediatricians lack knowledge about the needs of transgender and gender-diverse youth, they may default to the “watch and wait” approach. This method is outdated and harmful….” (The article does carry a footnote, "The views expressed in this article are those of the author, and not necessarily those of the American Academy of Pediatrics.)
America was fast to import and accelerate the European approach to treating minors, putting it “on steroids” and adding the scalpel. However, when it comes to reversing course, it intends to take its time. Why AAP staunchly refuses to accept the conclusions of multiple systematic reviews of evidence that found the practice of youth gender transition to either not be clearly beneficial, or net-harmful is unclear. Although the AAP has finally agreed to commission its own systematic review, it has already presaged the review's conclusion, which is that it will support the current pro-affirmation AAP position. In the meantime, thousands of American children and parents continue to be misinformed that science and evidence support the practice of gender transitions for youth who desire them, and that those raising concerns are merely science-deniers spreading “scientific misinformation” at best, and likely ill-intentioned. Therefore, it is not surprising that in America, the debate will continue to be politicized, and may ultimately be adjudicated in the court of law rather than due to the diligence and responsible actions and course corrections of the medical community itself, as is currently underway in Europe.
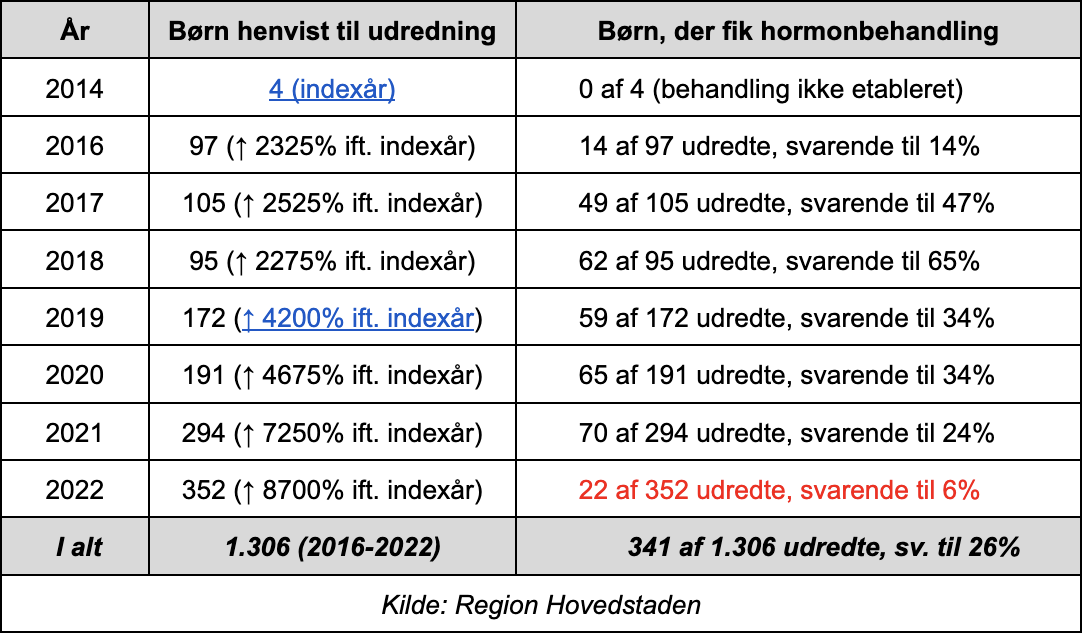
Intakes vs Approvals for Endocrine Interventions for Minors by Year, Denmark*:
Footnotes:
* The referrals and treated numbers for the Danish national gender clinic service are available at the Danish Rainbow Council website. While SEGM cannot independently verify the accuracy, we have no reason to doubt these statistics. Specifically, the number of referrals for 2016 (n=97) and 2022 (n=352) matches the data reported in this source and the numbers quoted in the referenced official Dutch medical journal. Official sources indicate that, "while approximately 67 percent of those referred were offered hormone treatment in 2016, this rate dropped to 10 percent of those referred in 2022."
** The speech by the Danish Minister of Health, Sophie Løhde, is available at this link. The English language transcript is available at this link.