False Assumptions Behind Youth Gender Transitions
The highly medicalized approach to managing gender distress in youth, integral to the “gender-affirmative” care model, rests on several key assumptions. Publications promoting “gender affirmation” of youth fail to explicitly call out these assumptions—or misrepresent these problematic assumptions as proven facts.
A recent publication by J. Cohn examines several key assumptions that underlie an influential “pro-affirmation” paper published by the prestigious journal, Nature. These assumptions permeate much of the “gender-affirming” literature more generally, including the most recent publication co-authored by the same author (Rosenthal). Cohn critically examines and cogently refutes each of the assumptions, observing that they range from entirely unproven to demonstrably false.
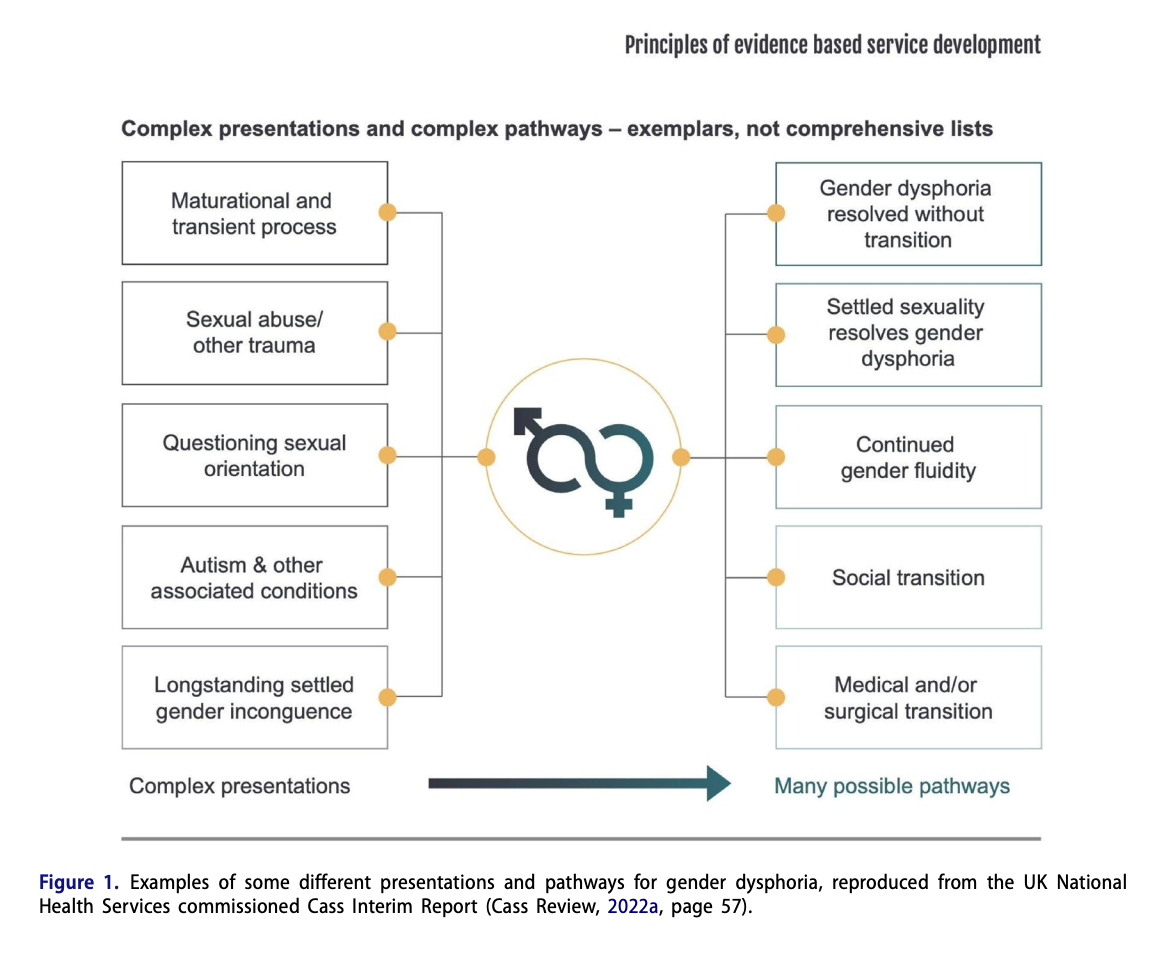
There are many causes of gender dysphoria – and many paths to resolution
Cohn draws attention to the fact that the “gender-affirmative” model of care continues to emphasize social, medical, and surgical interventions, despite the fact that several European countries (Sweden, England, Finland) now recognize the unfavorable risk/benefit ratio of this approach and recommend noninvasive approaches as first-line treatment. Quoting the recent review by Dr. Cass tasked with re-evaluating service delivery to gender dysphoric minors in England, Cohn draws attention to the fact that gender dysphoria has many different pathways and presentations, and that there is no consensus about best practices in terms of treatment.
Erroneous or unproven assumptions underlie the highly medicalized “gender affirmative” approach
Unproven assumption 1. Gender identity, which underlies gender dysphoria, is a fundamental personal characteristic that is biologically "ingrained."
This assumption is key to the entire concept of medical and surgical transition (“gender affirmation”) of minors. If gender dysphoria is biologically predetermined, immutable, and causes immense lifelong suffering, then intervening as early and aggressively as possible to “realign” the body with gender identity—even at the cost of lifelong dependence on exogenous hormones and future sterility—might be ethically justified.
However, Cohn observes that the assumption of a fundamental biologically ingrained “gender identity,” while intriguing, has never been proven, despite many attempts. For example, brain studies that purport to distinguish objective differences in brains of trans-identified individuals are highly flawed: the differences disappear once confounding factors such as sexual orientation (or exposure to exogenous hormones) are controlled for. Other studies rely on extremely small sample sizes, find nothing conclusive, or detect no signal.
Cohn also notes a common intellectual sleight of hand used by authors making the “biological case” for gender identity when they invoke studies of people with disorders of sexual development (DSD). People with DSD have demonstrable chromosomal and/or endocrine abnormalities. However, the vast majority of trans-identified individuals do not have DSD (and the vast majority of DSD individuals don’t suffer from gender dysphoria), so referencing DSD studies in order to claim a biological origin of gender dysphoria or trans identity is misleading.
The assumption of the core biological underpinning for “gender identity” and “gender dysphoria” remains an unproven theory: while biology likely plays a role in gender nonconformity, currently, there is no brain, blood, or other objective test that distinguishes a trans-identified from a non-trans identified person once confounding factors such as sexual orientation are controlled for. Further, the high rate of childhood desistance from gender dysphoria before maturity, (61-98%) and growing evidence of desistance among youth who developed gender dysphoria during or after puberty, challenge the notion that a biologically ingrained “gender identity” is responsible for gender dysphoria. This, in turn, suggests significant ethical problems with treating gender dysphoric youth with irreversible and potentially dangerous medical interventions. The Endocrine Society’s protocol (puberty blockers at the earliest stage of puberty, followed by cross-sex hormones) renders all those treated according to the protocol infertile or sterile, with no proven methods to preserve fertility due to immaturity of the gonads (ovaries and testes).
Unproven assumption 2. The sharp rise in the number of youth presenting with gender dysphoria does not signal a true increase in cases—it’s merely better detection.
Cohn notes the reluctance of “gender-affirmative care advocates” to acknowledge the meteoric rise in trans identification in youth that has engulfed much of the Western world since 2015. This baffling epidemiologic trend is either unacknowledged or is dismissed as merely “better detection” due to patient willingness to "come out" and growing physician awareness of the condition. While undoubtedly true in some cases, the notion that “better detection” alone is responsible for the several-thousand-percent rise in trans identification in youth is far-fetched.
Increasingly, an alternative theory that gender dysphoria may be a maladaptive coping mechanism rapidly spreading through social networks of vulnerable youth, posited by Littman, is viewed as much more likely. This is evidenced both, by the statements from several public health authorities alarmed by the sharp rise of trans identity in vulnerable youth, and by their sharp change in the treatment approach. England, Sweden, and Finland have replaced the "affirmative" model of medically altering the bodies of teens, with a non-medicalized, conservative treatment approach that prioritizes psychotherapy as the first line of treatment.
Cohn also notes the ongoing attempts by the proponents of "gender-affirming care" to discredit Littman's theory. To clarify, this theory, known as "ROGD" (rapid-onset gender dysphoria), and often understood as the "social contagion" theory (a well-established phenomenon in psychology), suggests that psychosocial factors such as trauma, mental health conditions, maladaptive coping mechanisms, and internalized homophobia, predispose youth to gender dysphoria, which can spread rapidly through social networks. Like all theories, it should be subjected to tests.
However, Cohn notes that the ROGD theory receives a consistently unscholarly, unfair, and biased treatment by the gender medicine establishment. For example, it is common for the proponents of "affirmation" to erroneously claim that Littman’s paper has been “debunked” or somehow proven wrong—a wrong claim that has been repeated in the Nature paper by Rosenthal. In fact, the highly influential paper by Littman (which has been viewed over 450,000 times and rated as #1 most-read scientific paper by PLOS ONE) was subjected to a second round of peer-review after publication, which led to a re-publication, but after 2 rounds of peer-review it emerged with its key conclusion of “social contagion” intact: “Other than the addition of a few missing values in Table 13, the Results section is unchanged in the updated version of the article.”
At the time of its publication, Littman’s paper was harshly criticized by the gender medicine establishment for its reliance on parental reports—despite the fact that parental reports are commonly relied on by health professionals for a range issues related to children’s health, and are commonly used by pro-affirmation clinicians themselves. Littman’s more recent research with patients (rather than parents), published in 2021, addressed the criticism: Affected patients themselves have now endorsed Littman’s ROGD theory when reflecting on their own experiences of how their trans identity developed.
Cohn notes that ROGD is unlikely to account for all the currently presenting cases of youth with gender dysphoria (and Littman’s research never made such a claim). However, the likelihood that ROGD plays a role in the genesis of gender dysphoria in a significant number of currently-presenting cases ethically threatens the notion that youth should be treated with irreversible body-modifying procedures—which is probably why the gender medicine establishment vehemently denies the increasingly self-evident importance of this theory.
False assumption 3. Medical interventions in gender-dysphoric minors have clear eligibility criteria.
When asserting that “gender-affirming” medical and surgical interventions are appropriate for minors, the proponents of this treatment pathway commonly add a key qualification: “for those who are eligible.” This implies the existence of clearly articulated eligibility criteria, which, when followed diligently, will lead to positive long-term health outcomes. Cohn observes that the reality is in stark contrast to this claim.
Eligibility criteria for medical gender affirmations in youth, as currently practiced in North America and most of the Western world, are opaque and vague. Medical interventions are initiated largely based on patient demand, which is in turn “affirmed” by “expert” pro-affirmation clinicians. Of note, when asked to explain their approach to differential diagnosis, assessment of patient prognosis, and criteria for recommending medical interventions, “gender-affirming experts” are frequently unable to articulate how they determine medical necessity.
Cohn also takes on a key misleading claim by proponents of gender affirmation, repeated in the influential Nature paper by Rosenthal, that adolescents with gender dysphoria will nearly certainty grow up to be transgender identified adults: “Longitudinal studies have indicated that the emergence or worsening of gender dysphoria with pubertal onset is associated with a very high likelihood of being a transgender adult.” Once again, Cohn notes an intellectual sleight of hand at play: This statement conflates two very different presentations of youth with gender dysphoria—that of early childhood-onset gender dysphoria persisting into adolescence, and a markedly different presentation of gender dysphoria that emerged for the first time during or after puberty. The statement in the Nature paper (above) is “supported” by a reference to the Dutch foundational research—however the Dutch researchers never made the claim that gender dysphoria emerging in adolescence is likely to persist into adulthood.
The Dutch researchers did posit that gender dysphoria that starts from “toddlerhood on” and persists and worsens during adolescence is likely to persist life-long. This potentially credible theory, based on expert opinion of the Dutch research team, remains a theory since it has never been tested (and some of the early Dutch research appears to challenge this theory, demonstrating that the majority of adolescents rejected from medical intervention actually desisted before reaching mature adulthood). However, this type of early childhood-onset of gender dysphoria is quite different from instances when gender dysphoria emerges around adolescence for the first time. Contrary to Rosenthal’s claim, the Dutch researchers were quite concerned about medically treating youth with pubertal onset of gender dysphoria, and delayed their transition until adulthood precisely because they were concerned that trans identity in such youths may be transient. Most recently, the principal investigator of the Dutch protocol explicitly stated that such cases may need different treatment and that psychotherapy may be more appropriate than hormones and surgery for these patients.
Playing fast and loose with citations to bolster the “pro-affirmation” narrative, evident in the Nature review by Rosenthal, is a common tactic among gender-affirmation advocates, and it has been noted by other researchers. Readers and peer-reviewers are well-advised to always check the references before assuming that the citations support the claims that underlie the increasingly-disputed science of “gender-affirming care.”
False assumption 4. Medical interventions for gender dysphoric minors have been demonstrated to be safe and effective.
Cohn notes that although the WPATH guidelines imply safety and efficacy, these guidelines are based on very low-quality evidence. Contrary to assertions of gender-affirmation advocates that “very low/low quality evidence” merely means a lack of randomized controlled studies, this designation signals that the results reported by the studies in the field warrant very low confidence and are generally not trustworthy, due to problems in study design and execution, and/or poor generalizability of results to currently presenting populations.
Cohn notes that a recent overview of systematic reviews of evidence (also known as an "umbrella review") concluded that “(t)he available medical literature provides insufficient evidence that sex reassignment through medical intervention is a safe and effective treatment for gender dysphoria.” This "umbrella review" accurately summarizes the findings of existing English-language systematic reviews of evidence, such as a recent Cochrane systematic review, which “found insufficient evidence to determine the efficacy or safety of hormonal treatment approaches for transgender women in transition,” and the UK systematic review of evidence, which came to even more stark conclusions. The UK NICE reviews concluded that puberty blockers did not improve mental health, while cross-sex hormones showed some improvements but they were uncertain and have to be balanced with potentially serious health risks. Other non-English-language systematic reviews of evidence that were not included in the "umbrella review," such as the ones from Sweden, and Finland, reached similar conclusions that the risks of "medical affirmation" likely outweigh the benefits for most currently affected youth.
Cohn observes Rosenthal’s seeming disregard of the implications of risks to sexual function and fertility, as well as risks to bone and cardiovascular health, directly caused by or associated with medical interventions. Other researchers have also noted that those advocating for medical “gender-affirmation” of minors tend to trivialize the risks, erroneously likening them to the risks of taking an occasional aspirin for a headache.
Unproven assumption 5. Detransition does not represent medical harm and is rare.
The growing reports of medical detransition and regret highlight the problem of wrongful gender transitions of youth. When faced with the statistics, such as recent evidence of 10-30% of medical detransition among young people after a relatively short period of time, as well as detransitioners’ own reports of regret, gender-affirmative clinicians tend to dispute these numbers or recast detransition as a benign “gender journey.”
Cohn emphasizes that studies that purport very low rates of regret are deeply flawed and unreliable. For example, the study frequently quoted as evidence for 1% regret rate, referenced by Rosenthal, would not have counted Keira Bell as a regretter. Bell is arguably the most famous detransitioner and regretter from the novel cohort of youth, and her case had set in motion a process that will culminate with the 2023 closure of UK’s pediatric gender clinic. More generally, England has disavowed the medical “gender-affirmative” treatment pathway for most youth, and is replacing this care model with non-invasive, developmentally-informed approaches as first line of treatment.
The study used by Rosenthal to claim the 1% regret rate deserves special attention, as it exemplifies problems in the "low regret" research. This study used a very narrow definition of regret: the subjects had to return to the same clinic that medically treated them and explicitly verbalize regret, which would then have to have been documented and their medical chart—and they would also have to start supplementation with natal sex hormones from the same gender clinic. This explains why someone like Keira Bell—who “only” received hormones and a mastectomy, but had no gonadectomy (removal of ovaries) and did not need same-sex hormonal supplementation—would not be counted as a “regretter.” In addition, the researchers could not assess outcomes for 36% of the initial cohort since they ceased their contact with the clinic.
Cohn alerts readers that reports of detransition are increasing in frequency, and those asserting low regret rates rely on inaccurate estimates due to premature measurements of outcomes, inappropriate measurement instruments, and sample biases. Cohn reiterates, “regret underestimates are also likely because patients might not inform their clinicians; only 24% of detransitioners in Littman’s (2021) convenience sample did so,” and avers that detransition has the potential to “cause distress and even devastation.”
Conclusion
Cohn reminds us that oft-repeated inaccuracies can erroneously harden into “facts,” misleading clinicians and patients alike. Cohn concludes, “There are serious challenges in deciding how to best support those currently suffering from gender dysphoria, given how little is known about this complex condition. Accurately describing what the evidence currently says and does not say, and what further evidence is needed, is crucial.”